














 25 / 48
25 / 48

25
Volume 3 Issue 5
|
I
ssues and
P
eople
Resume comprehensive risk management care
Printedwithpermissionof IanMcConnachie,DDS,MS,FRCD(C)
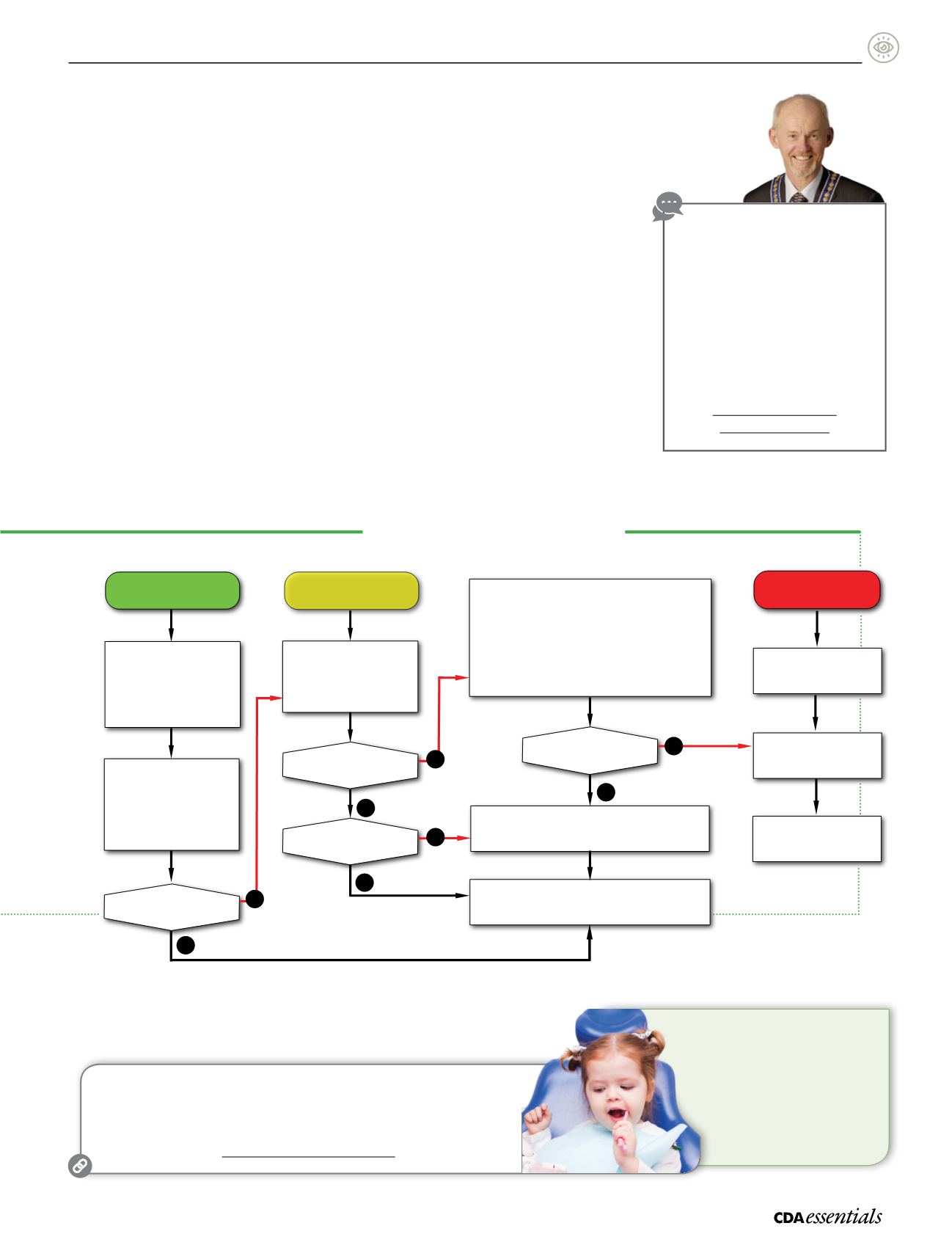
Risk Management Algorithm
Early Childhood Caries
Anticipatory Guidance
Diet
Growth and development
Commitment to appropriate
periodicity of o ce care
Motivational interviewing
Low Risk
High risk:
cavitated lesions
Moderate to high risk:
non-cavitated lesions
Reduced periodicity and
treatments:
Annual visits
Introduction to prophylaxis
as child development
progresses
X-rays required at a later date
Patient status deteriorates?
Assess for:
Anti
microbials
– Topical fluoride
– Sealants
– Appropriate p
eriodicity
Patient becomes high risk?
Restoration need
ed?
Staged care:
Systematic desensitization
Antimicrobials
Topical uoride
– Atraumatic restorative treatment (ART)
Glass ionomer (GI) sealants
Appropriate periodicity
(May include initial sedation visit(s) to control pain and infection.)
Unstable clinical situation?
Permanent restoration with or without sedation
Staged care while waiting
for general anesthesia
*Decision to treat or refer can come at any stage.
Treatment under
general anesthesia
Completion of
restorative treatment
Yes
No
No
No
No
Yes
Yes
Yes
The elements of the first dental visit are broad and
build important links:
Parent interview
Assessment of parental motivation
Visual exam to assess risk
Development of a risk management protocol
Oral hygiene instructions
Application and dispensation of preventive
therapies
“Having examined the child and taken in the
relevant information, we can position them into
the most appropriate risk category using one
of the assessment models available, with the
3 general categories being low risk, moderate
to high risk (non-cavitated lesions), and high risk
(cavitated lesions),” adds Dr. McConnachie.
Risk management
“As care providers, we need to first decide how
far into the algorithm we are comfortable going,
and at what point we need to refer to another
clinician—and this obviously includes building
a relationship with the pediatric
specialist, consistent with our
own philosophy of care,”
emphasizes Dr. McConnachie.
Dr. McConnachie encourages
dentists to take the plunge
and treat young patients: “Start
slowly. Get comfortable with the
lower-risk patients. Start with
the first exam by first birthday.
Build skills. Always have a plan B,
and be prepared to enjoy the
experience!”
a
Visit
Oasis Discussions
to
watch a video interview with
Dr. McConnachie.
The video includes an overview
of Dr. McConnachie’s algorithm
for ECC risk assessment
and management, and
the presentation of
ECC risk-management cases.
oasisdiscussions.ca/2015/06/09/eccp
Share Your Experience
Do you see infants in your practice?
Have you adopted a risk management approach to ECC?
Send your feedback to
oasisdiscussions@cda-adc.caor call 1-855-716-2747.
Forourreaders inOntario, further informationon
thistopicwasrecently featured in
OntarioDentist
magazine:
McConnachie, I.Newsolutions forgeneral
practitioners intreatingearlychildhoodcaries.
OntarioDentist.
2016;93(2):23-25.
McConnachie, I.Stagedcare–newsolutions
fortreatingearlychildhoodcaries.
OntarioDentist.
2016;93(3):32-36.